It's nice when you see a new paper describing the type of science that you find the most exciting and relevant, and doubly so when it's written by a group of people that you know and respect. Full disclosure: this paper is from the group that I did my graduate work with at the University of Pennsylvania, and there's quite a lot to talk about.
Building a model for microbiome research
Before talking about what the authors did, I want to describe how they did it. They started (in a previous study) with a cohort of patients being treated for a common disease with no known cure (Crohn's) and looked for differences in the genomic content of their microbiome compared to healthy control subjects. That initial analysis indicated that one particular metabolic pathway was enriched in patients with the disease. In this study they followed up on that finding by analyzing the metabolites produced by those microbes. The combination of those two orthogonal analyses (genomic DNA and fecal metabolites) provided some suggestion that microbes in the gut were producing one particular chemical which may have a role in disease. To test that hypothesis they moved into a mouse model where they could test that hypothesis with controlled experiments, not only adding and removing microbes but also tracking the passage of metabolites via isotopic labelling. That model system provided crucial data that supported the findings from the human clinical samples – that a specific bacterial enzyme may have a role in human disease. After this study, I can only imagine that the next step would be to move back into humans and see if that target can be used to generate a useful therapeutic.
The microbiome field is relatively new, and I believe that its first batch of groundbreaking therapeutics is just over the horizon. I wouldn't be surprised if the most influential studies in this field follow a trajectory that is similar to what I describe above: generating hypotheses in humans, testing them in animal models, and moving back to human to test and deliver therapeutics.
Ok, enough predictions, let's get into the paper.
The Microbiome – Who's Who and What's What

Fig. 2. Associations between bacterial taxa abundance ascertained by fecal shotgun metagenomic sequencing and the fecal metabolome in healthy pediatric subjects and those with Crohn’s disease.
The figure above shows the association between Who's in the microbiome (bacterial genera, vertical axis) and What's (metabolites, horizontal axis) in the microbiome. The point here is that certain microbes are associated with certain metabolites, with a big focus on the amino acids that are being produced. The prior set of experiments suggested that the microbes in Crohn's patients had an increased capacity for producing amino acids, while this figure (and Figure 1) goes further to show that there is a subset of microbes associated with higher actual levels of amino acids in those subjects.
Tracking metabolism in the microbiome
Here's a deceptively simple figure describing a powerful finding.
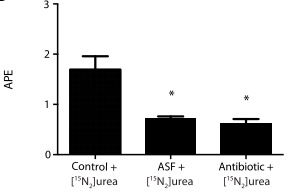
Fig. 3. In vivo heavy isotope assays using 15N-labeled urea to determine the effect of bacterial urease on nitrogen flux in the murine gut microbiota.
This experiment uses radiolabelled urea to measure the production of lysine by microbes in the gut. The central question here is what is producing the extra amino acids in Crohn's disease? In this experiment the authors added radiolabelled urea so that they could track how much lysine was being produced from that urea. Crucially, they found that adding either antibiotics or a defined set of microbes (called "ASF") reduced the amount of lysine that was produced from that urea, which supports the hypothesis that microbes in the gut are directly metabolizing urea.
Tying it all together

Fig. 6. Effect of E. coli urease on colitis in a T cell adoptive transfer mouse model of colitis
I've skipped over a lot of interesting control experiments so that I could get to the grand finale. Everything I've told you up until now has established that (a) Crohn's patients have higher levels of certain amino acids in their stool, (b) those high amino acid levels are associated with particular bacteria, and (c) bacteria in the gut are able to produce amino acids from urea. To bring it all together the authors went to a mouse model of colitis to see whether adding or removing a single gene would have an effect on disease. They found that E. coli with urease (an enzyme that metabolizes urea) caused significantly more disease than E. coli without urease. This brings it all back to the action of a single gene on a model of human disease, which is the classic goal of reductionist molecular biology, but the gene of interest is encoded by the human microbiome.
I think that's pretty cool.
From here it's easy to imagine that people might be interested in designing a drug that targets microbial urease in order to reduce human disease, although that's got to be a pretty difficult task and I have no idea how diverse bacterial urease enzymes are.
Bringing it back to my first point, this seems like the best case example of how to advance our understanding of the human microbiome with the goal of treating human disease. I hope to see many more like it in the years to come.